























Medical Disclaimer
Medical Disclaimer: This text is intended for educational purposes only and does not substitute for professional medical evaluation or treatment. Every clinical decision must account for patient history, comorbidities, infection severity, microbiology data, and local antimicrobial resistance patterns.
Author: Charles D. Goff, MD, FACS
Introduction
Soft tissue infections are among the most frequent postoperative and traumatic complications treated in U.S. surgical practice. With antimicrobial resistance evolving quickly, antibiotic selection in SSTI treatment has become a strategic and outcome-defining decision. An effective drug halts systemic escalation, prevents necrosis and accelerates healing. An ineffective one can allow infection to penetrate fascia, enter bloodstream circulation or progress to osteomyelitis. For a surgeon in 2025, the ability to differentiate appropriate and inappropriate antibiotic coverage is no longer optional it is critical to patient survival and tissue preservation.
This article analyzes three commonly referenced agents Flagyl (Metronidazole), Zithromax (Azithromycin) and Erythromycin comparing their spectra, clinical relevance and appropriate usage scenarios. The goal is to guide practical bedside decision-making, not produce theoretical pharmacology. By the end the reader will understand when macrolides are acceptable, when Flagyl is mandatory and when neither option is safe, requiring escalation toward broader agents such as doxycycline, TMP-SMX or combination therapy.
Soft Tissue Infection Pathogens and Why Correct Antibiotic Matching Matters
Soft tissue infections differ from simple dermatologic irritation. Once bacteria enter subcutaneous layers or fascial planes, replication accelerates and tissue oxygenation decreases, creating conditions for anaerobic colonization. In the U.S., most basic cellulitis cases still originate from Streptococcus spp. and MSSA, yet the present decade shows a marked upward trend in community-acquired MRSA, recurrent infections in diabetics, and mixed aerobic-anaerobic postoperative wounds.
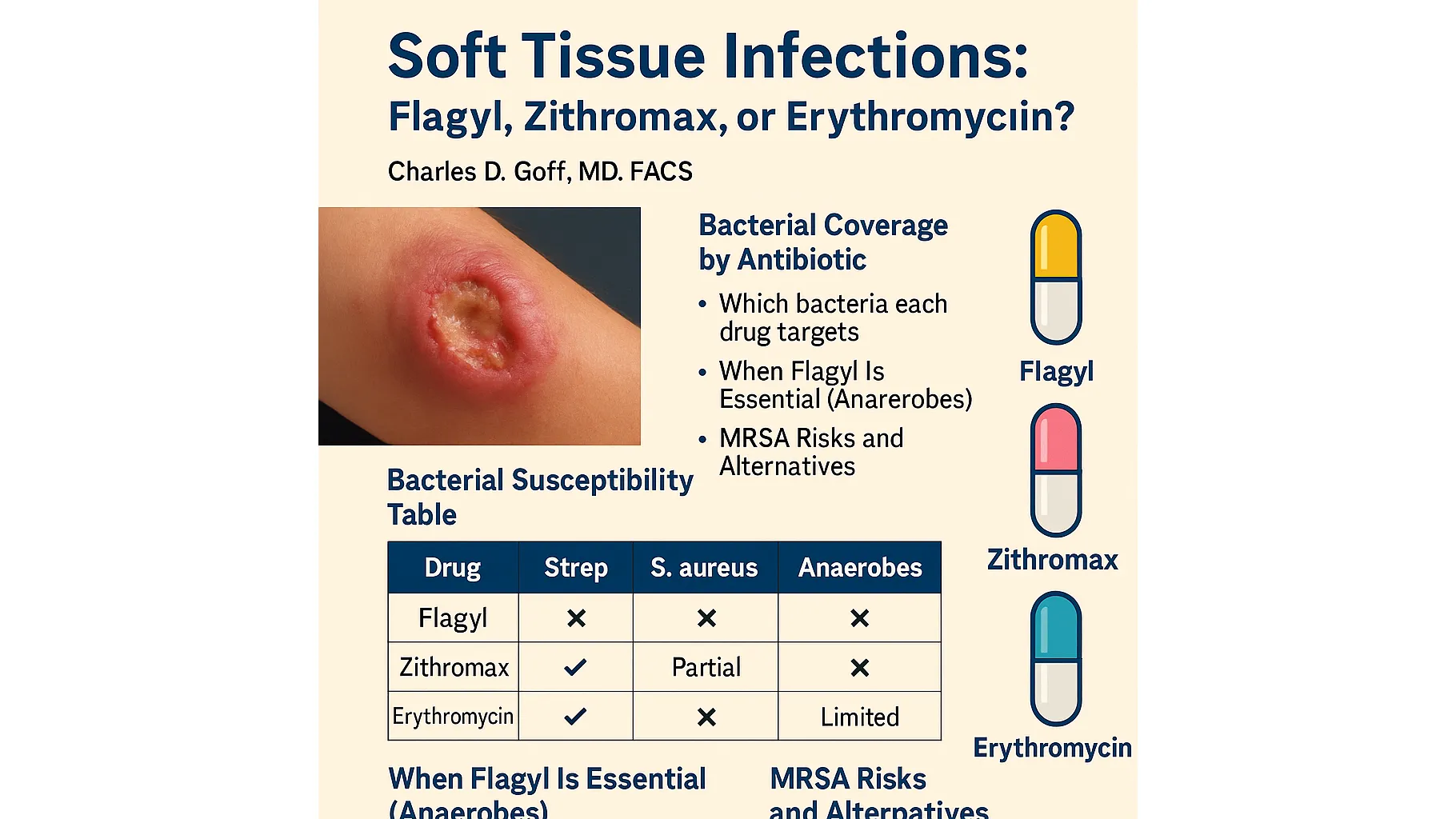
A surgeon makes therapeutic decisions based not just on culture, but on probability and risk profile at presentation. The following table illustrates coverage differences clearly, showing where each drug succeeds and fails:
| Drug | Streptococcus Coverage | S. aureus (MSSA) | Anaerobes | MRSA |
|---|---|---|---|---|
| Flagyl (Metronidazole) | No | No | Strong | No |
| Zithromax (Azithromycin) | Good | Weak / Unreliable | No | Not recommended |
| Erythromycin | Good | Weak | No | Ineffective |
From this comparison, the emphasis becomes unmistakable:
- Flagyl is the only agent in this trio with clinically meaningful anaerobic activity.
- Macrolides are acceptable only in mild non-MRSA aerobic SSTI.
- Neither Zithromax nor Erythromycin should be used for MRSA-suspected infections.
- If infection type is misjudged, failure is predictable.
Flagyl (Metronidazole): The Essential Anaerobic Antibiotic for Deep and Necrotic Infections
Flagyl plays a foundational role in modern surgical infectious disease management. Its tissue penetration in oxygen-poor environments makes it indispensable for anaerobic soft-tissue infections, particularly where necrosis or drainage is present. Anaerobes thrive where vascular supply is weak deep surgical cavities, chronic diabetic ulcers, bite wounds, pressure injuries. Macrolides do not reach therapeutic strength in these zones. Flagyl does.
Clinical scenarios strongly suggesting anaerobic involvement include:
| Presentation Indicator | Interpretation |
|---|---|
| Foul smell or necrotizing edges | Anaerobic overgrowth likely |
| Thick or dark purulence | Reduced oxygen perfusion |
| Postoperative cavity with tissue sloughing | Mixed flora probable |
| Human/animal bite | High anaerobic composition |
When such features appear, Flagyl is not optional it is required. Zithromax and Erythromycin lack anaerobic activity entirely. Using them in deep necrotic wounds is not just clinically unsound it increases progression risk and complicates surgical salvage. In polymicrobial infections, Flagyl is often combined with a second agent to cover aerobes, giving surgeons full-spectrum protection where single-drug therapy would fail.
Zithromax and Erythromycin: Limited but Valid Use in Mild Aerobic SSTI
Macrolides occupy a narrow but clinically real space. When an infection is mild, superficial and dominated by Streptococcus species, and when penicillin cannot be prescribed, Zithromax (Azithromycin) or Erythromycin may be useful. Oral dosing improves adherence and makes them suitable for outpatient follow-up. They are not broad surgical antibiotics they are targeted tools.
However, macrolides should never be selected empirically in suspected MRSA cases. They also do not treat anaerobic infections. This limitation makes them inappropriate for abscessing, necrotizing or deep tissue involvement.
Where Zithromax is considered first-line today
- Low-risk cellulitis without purulence
- Early superficial infection with rapid monitoring
- Documented non-MRSA streptococcal etiology
Even in those cases, resistance trends require caution, and therapy must be reassessed if clinical response is not visible within 48–72 hours.
MRSA in 2025: Why Macrolides Are No Longer Safe Empiric Therapy
The greatest shift in soft-tissue infection management over the last decade has been the surge in community-acquired MRSA. Ten years ago, this organism was primarily hospital-associated. In 2025, it is frequently seen in athletic environments, household transmission clusters, school settings and recurrent wound cases. The presence of MRSA risk factors fundamentally changes antibiotic selection. Where standard streptococcal cellulitis once responded well to macrolides, modern clinicians now face strains that carry high-level macrolide resistance.
That means Zithromax and Erythromycin are poor empirical choices when purulence, abscess formation or treatment failure history is present. Even when culture is pending, delayed adjustment can result in rapid progression. MRSA spreads along fascial planes faster than traditional MSSA, and monotherapy with macrolides has been repeatedly documented to fail before day three of treatment.
Clinical predictors of MRSA
Antibiotic selection must shift based on presentation rather than waiting for culture results. A typical MRSA infection presents as:
- Worsening pain out of proportion to erythema
- Purulent drainage or abscess structure
- Recurrent SSTI within the last 90 days
- History of MRSA in household contacts
- Rapid failure of outpatient macrolide therapy
In these situations, MRSA-active therapy is required from the beginning. Neither Azithromycin nor Erythromycin possesses reliable activity against resistant Staphylococcus aureus, and Flagyl offers none. That means none of the three evaluated antibiotics are appropriate as monotherapy where MRSA is probable. At this decision point, escalation is indicated – and the recommended direction is outlined in article№13, dedicated to Doxycycline as an MRSA-effective alternative.
Decision Pathway for Surgeons: A Practical Antibiotic Selection Algorithm
Step One – Is the infection superficial with clear streptococcal presentation?
If erythema is diffuse, without necrosis, without abscess and the patient is otherwise stable, macrolides may be considered. In this narrow scenario, Zithromax remains a viable alternative for patients with penicillin intolerance. However, adequate follow-up must be scheduled. Lack of visible improvement within 48–72 hours indicates misclassification or early resistant involvement.
Step Two – Is necrosis, odor or deep purulence present?
When tissue oxygenation is reduced, bacterial behavior changes. In this environment, anaerobes dominate and macrolides fail reliably. Flagyl becomes mandatory, often as part of combination therapy. Surgeons treating bite wounds, postoperative cavities or diabetic plantar breakdown cannot rely on macrolides, even if symptoms appear initially mild. Delay worsens outcome.
Step Three – Is there purulence, abscess or rapid progression?
These hallmarks indicate potential MRSA, and macrolides are unsafe. If a patient presents after a failed outpatient course of Zithromax, erythromycin or cephalexin, resistant staphylococcal components should be assumed until proven otherwise. In such cases, escalation is not optional it is standard of care. This is why many surgeons shift directly to tetracycline-class agents or dual therapy.
Step Four – Consider surgical management as co-treatment
No antibiotic can substitute for incision, irrigation or debridement when there is structural infection. Drainage reduces bacterial load, improves oxygenation and increases antibiotic penetration. In this context, Flagyl or macrolides are supporting tools not replacement for physical intervention.
Combination Therapy: Where One Antibiotic Is Not Enough
Deep soft-tissue infections are frequently polymicrobial, especially in wounds that involve organic exposure, bites or surgical site compromise. In these cases, no single agent from the three under review is sufficient. A surgeon may combine Flagyl with another antibiotic to provide comprehensive coverage of both anaerobic and aerobic flora.
Below is a breakdown of combination logic:
| Clinical Situation | Preferred Approach | Why |
|---|---|---|
| Anaerobic infection with aerobic component | Flagyl + agent with aerobic coverage | One class cannot cover both spectra alone |
| Deep postoperative wound with necrosis | Flagyl cornerstone + escalation drug | Surgical penetration and oxygen gradient demand spectrum expansion |
| Recurrent MRSA with abscess | Macrolides avoided; escalate to MRSA-active therapy | Resistance failure is predictable with azithromycin |
Macrolides alone cannot support necrotic or MRSA-driven infections, but they may contribute to combination therapy where targeted streptococcal suppression is needed after debridement.
When None of the Three Drugs Should Be Used
As severity increases, antibiotic selection must evolve beyond these three choices. There are clinical situations where Flagyl, Zithromax and Erythromycin are all inappropriate, including:
- Rapid systemic involvement
- Gas-forming tissue infection
- Hemodynamic instability
- Extensive anaerobic-mixed necrosis
- Culture-confirmed MRSA nonresponsive to monotherapy
In these cases, surgeons step outside the initial drug set entirely. Management shifts toward broader-spectrum therapy and inpatient monitoring.
When Escalation Is the Only Safe Choice
Surgeons confronting aggressive soft tissue infections understand that delay not severity causes limb loss. The earlier the antibiotic gap is recognized, the greater the probability of salvage. When Flagyl does not resolve anaerobic progression, or when macrolides cannot suppress aerobic dominance, escalation is no longer optional. The clinician must step outside the three-drug comparison and select therapy with broader reach.
This scenario most often arises in:
- rapidly expanding erythema
- bullae formation or skin separation
- necrotic tissue undermining
- systemic fever, leukocytosis and CRP acceleration
- pain exceeding clinical appearance
In these conditions, standard outpatient macrolide therapy is inadequate. Flagyl alone is insufficient because anaerobes are seldom the only pathogens present. Clinical judgment must shift toward dual-drug regimens or MRSA-focused therapy. Mixed pathogens require mixed solutions. Single-mechanism therapy works only before the infection multiplies across layers of fascia and fat. After that threshold, escalation determines outcome.
For vascular-compromised limbs, diabetic ischemia, or tissue breakdown resulting from poor perfusion, the clinical logic differs significantly. These cases benefit from advanced evaluation described in article vascular-origin soft tissue infection strategy
Antibiotic Strategy Matrix for Surgeons in 2025
To consolidate the full comparison into actionable structure, the treatment map below translates clinical presentation into recommended antibiotic direction. It is not a replacement for culture interpretation, but it allows the surgeon to respond decisively in the first treatment window.
| Clinical Presentation | Recommended Class | Rationale |
|---|---|---|
| Mild superficial cellulitis, likely Streptococcus | Macrolide (Zithromax/Erythromycin) with monitoring | Aerobic gram-positive dominance without MRSA risk |
| Deep cavity, foul odor, necrotic borders | Flagyl-based therapy mandatory | Anaerobic bacteria require Metronidazole penetration |
| Purulence or abscess formation | Avoid macrolides; consider MRSA-directed therapy | Resistant staphylococci common; macrolide failure expected |
| Bite wound, postoperative deep infection | Flagyl + aerobic coverage pair | Mixed flora predictable; monotherapy unsafe |
| Rapid systemic signs or deterioration | Escalation beyond reviewed drugs | Avoid undertreatment; prevent necrotizing spread |
The matrix is simplistic intentionally. Clinical execution must be decisive, not tentative. Over-analysis without therapeutic adjustment is a common failure point. In SSTI medicine, indecision is infection’s greatest ally.
Surgical Management as Equal Partner to Antibiotics
No antibiotic performs well inside a closed abscess chamber. Drainage, irrigation and tissue debridement remain non-negotiable components of soft tissue infection treatment. Surgeons who rely on pharmacology alone even with appropriate antibiotic choice may still witness progression because medication cannot diffuse through pus layers or necrotic slough.
When incision and drainage are combined with correct antibiotic coverage, outcomes transform. Necrotic tissue removal restores oxygenation, which inhibits anaerobic growth directly. Vascular access improves, allowing Flagyl or MRSA-directed agents to reach viable tissue margins. This dual-modality strategy forms the modern backbone of salvage surgery.
Macrolides may serve a role post-debridement if streptococcal colonization persists at the wound interface, but they should not be used as primary therapy in deep or purulent infections. Their function is adjunctive, not foundational. Flagyl, likewise, is not a complete system. It is a half-spectrum tool requiring an aerobic companion when polymicrobial attack is active. The surgeon’s focus, ultimately, must move beyond solo-agent thinking.
Final Clinical Conclusions
Flagyl, Zithromax and Erythromycin remain familiar drugs, but their appropriate usage has become more sharply defined in 2025. In soft tissue infections, macrolides are no longer broad-spectrum solutions. They are niche agents best reserved for mild, non-purulent cellulitis where Streptococcus is the clear dominant pathogen. They fail where MRSA or anaerobes exist and those organisms now appear with regular frequency.
Flagyl, in contrast, is the single effective tool in anaerobic invasion. It is indispensable in necrotic, deep, foul-draining wounds, in bites, and in oxygen-compromised postoperative tissue. However, Flagyl alone is not a complete defense. It requires pairing whenever polymicrobial involvement is likely.
The strongest predictor of success is not which drug is chosen, but how early misclassification is corrected. Surgeons must treat anaerobes with Flagyl, streptococci with macrolides selectively, MRSA with escalation medications, and deep infections with both pharmacology and steel. Delay, not bacteria, is the enemy.
Frequently Asked Questions (FAQ)
Can Zithromax be used for soft tissue infections in 2025?
Yes, but only for mild superficial cellulitis without MRSA risk or anaerobic involvement. Lack of improvement within 72 hours requires reassessment.
When is Flagyl the correct first-line choice?
When necrosis, foul odor, deep cavity, or bite-origin infection suggests anaerobic growth. Macrolides cannot substitute in these cases.
Do macrolides work for MRSA wounds?
No. MRSA carries high macrolide resistance. Zithromax and Erythromycin are considered unsafe empiric therapy in purulent infections.
Can Flagyl treat Staphylococcus aureus or streptococcal infections?
No. Its spectrum is anaerobic-dominant. It must be paired with another drug when aerobic bacteria are present.
When should escalation beyond these three antibiotics occur?
When progression is rapid, drainage is required, MRSA is suspected, or mixed anaerobic-aerobic infection is deep. Escalation prevents systemic failure.