























Flagyl as the Standard for Anaerobic Coverage
Disclaimer
This article is intended for informational purposes and does not constitute medical advice. Antibiotic therapy must be prescribed only after direct evaluation by a qualified healthcare professional. Inaccurate or self-directed antibiotic use may lead to complications or treatment failure.
Author: William L. Faulkenberry II, MD, FACS
Why Flagyl Remains the Cornerstone for Anaerobic Abdominal Infections in 2025
Metronidazole(Flagyl) has maintained its position as the primary agent for anaerobic infections of the abdominal cavity for more than three decades, and updated 2025 clinical guidelines continue to support its central role.
The reason is straightforward: anaerobic bacteria remain a dominant force in infections that follow perforation of the gastrointestinal tract, abscess formation, necrotizing processes, and postoperative complications involving bowel contamination.
Bacteroides fragilis, the most clinically relevant anaerobe in abdominal infections, retains high susceptibility to metronidazole in nearly all surveillance datasets published between 2022 and 2024.
Unlike many broad-spectrum antibiotics, Flagyl offers precision rather than excess.
It does not affect Gram-positive aerobes, Gram-negative aerobes, or skin flora organisms that are common in soft-tissue surgical infections but far less relevant in abdominal sepsis.
This narrow targeting allows clinicians to combine Flagyl with other agents when the infection is polymicrobial, creating a regimen tailored to abdominal microbial ecology rather than relying on unnecessarily broad therapy.
With increased focus on antimicrobial stewardship, 2025 protocols emphasize using narrow-spectrum agents whenever possible.
Because metronidazole precisely covers the organisms of concern while sparing commensal flora, it remains a model example of responsible antibiotic prescribing in abdominal surgery.
The Anaerobic Microenvironment of the Abdomen
Anaerobic infections arise predominantly when the integrity of the gastrointestinal tract is compromised.
The colon contains some of the highest concentrations of anaerobes found anywhere in the human body, and even small perforations rapidly introduce these organisms into peritoneal spaces where oxygen tension is low enough to support their proliferation.
In these conditions, Bacteroides, Clostridium, Fusobacterium, and Peptostreptococcus species become dominant contributors to infection.
The distribution of anaerobes varies by anatomical site.
The small intestine contains far fewer obligate anaerobes, while the colon harbors dense communities capable of generating severe infections within hours of contamination.
This microbial gradient is essential when planning antibiotic therapy; for example, a perforated duodenal ulcer often requires a different coverage profile than perforated sigmoid diverticulitis.
Updated susceptibility reports from 2024 show that anaerobes remain predictably sensitive to metronidazole, with only isolated cases of resistance reported worldwide.
This stability contrasts with rising resistance patterns to macrolides, clindamycin, and certain cephalosporins.
As a result, choosing Flagyl early in the course of abdominal sepsis remains both evidence-based and clinically justified.
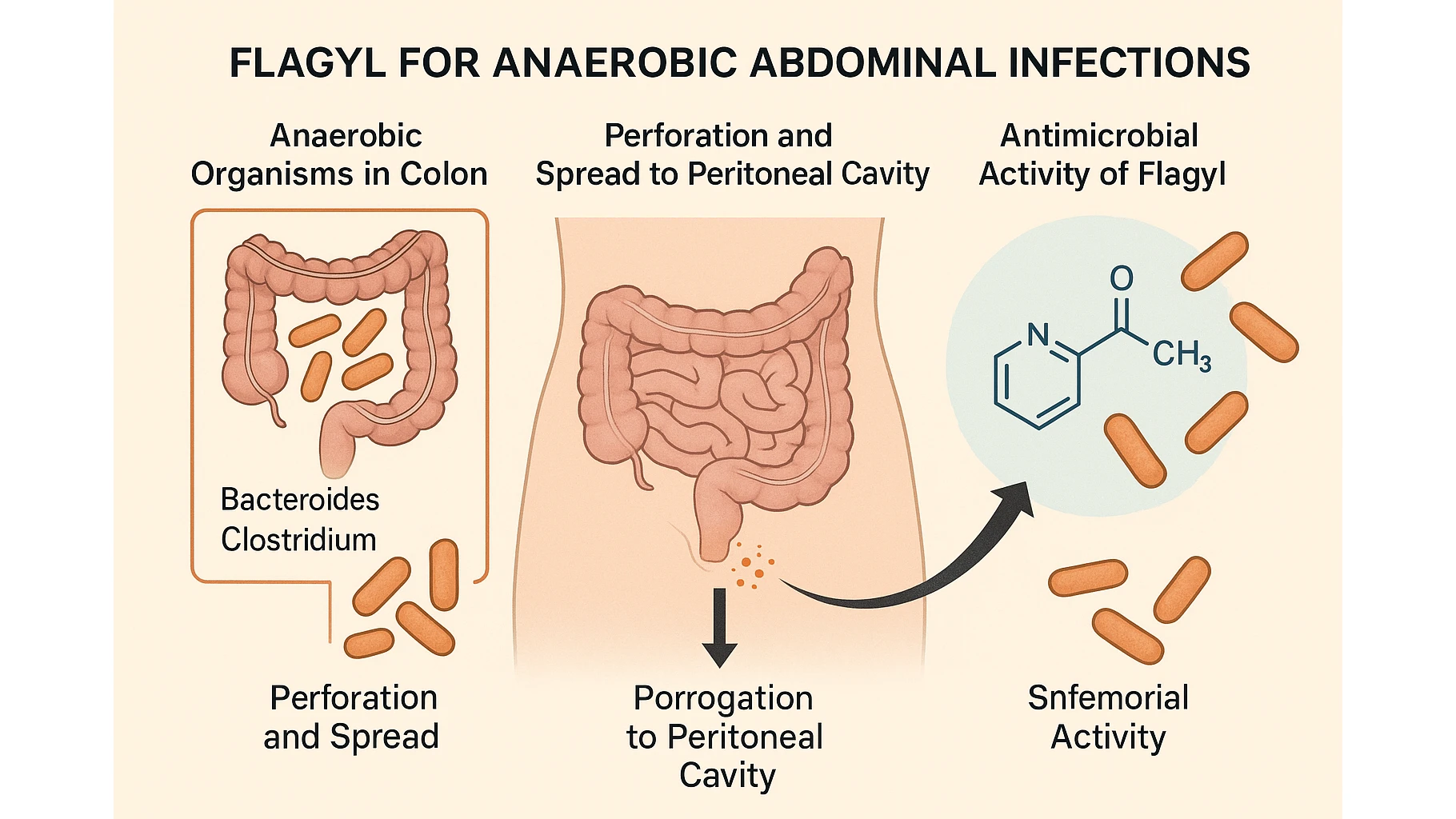
A clear visual representation of intestinal flora helps explain why anaerobic pathogens dominate abdominal infections.
The colon’s low redox potential, nutrient density, and minimal oxygen exposure create ideal conditions for obligate anaerobes, making them the primary microbiological target in nearly all perforation- or contamination-related abdominal emergencies.
When Flagyl Is Essential in Surgery
Flagyl becomes indispensable whenever a surgical infection originates from a breach in gastrointestinal continuity.
Perforated appendicitis, diverticulitis with abscess formation, colonic perforation, postoperative leaks after bowel anastomosis, and secondary peritonitis all require coverage directed at anaerobes.
In these cases, metronidazole forms the foundational component of modern antimicrobial protocols.
The drug’s role is equally critical in postoperative abdominal abscesses.
These infections typically contain mixed flora, including anaerobic species that will continue to proliferate even when broad Gram-negative agents are used.
Without adequate anaerobic coverage, clinical improvement is delayed and the risk of systemic deterioration increases.
Flagyl is also essential in necrotizing infections originating in the abdomen, where anaerobic organisms contribute to gas formation, rapid tissue destruction, and systemic toxicity.
Even when surgeons opt for aggressive broad-spectrum combinations, metronidazole remains a non-negotiable element of therapy because alternative agents rarely provide the same degree of predictable anaerobic suppression.
When Flagyl Is Not Enough: The Limits of Monotherapy
Despite being the cornerstone of anaerobic coverage, Flagyl has a deliberately narrow spectrum.
It offers no activity against aerobic Gram-negative organisms such as E. coli, Enterobacter, or Klebsiella, and does not cover aerobic Gram-positive organisms like streptococci or staphylococci.
These bacteria frequently coexist with anaerobes in bowel perforations, postoperative leaks, and secondary peritonitis.
As a result, monotherapy with Flagyl in abdominal sepsis leaves major components of the infectious process untreated.
Multiple observational studies from 2021–2024 demonstrate delayed clinical improvement when Flagyl is used alone in polymicrobial abdominal infections.
Persistent fever, rising inflammatory markers, and unresolving abscesses are common consequences of incomplete coverage.
For this reason, current protocols emphasize pairing Flagyl with an agent that reliably covers Gram-negative aerobes.
Misuse becomes especially apparent when cephalexin or similar narrow-spectrum agents are selected for abdominal infections.
Cephalexin provides neither anaerobic nor Gram-negative activity, a mismatch detailed extensively in article Keflex in Modern Surgery, where its limitations in deep or contaminated infections were analyzed.
In abdominal settings, improper substitution of Flagyl or omission of Gram-negative coverage can prolong hospitalization and increase the need for re-intervention.
Evidence-Based Combination Therapy in 2025
Modern management of abdominal infections relies on structured combination therapy.
Flagyl functions as the anaerobic backbone, while a complementary agent addresses aerobic Gram-negative organisms.
Flagyl Combination Table (2025)
| Clinical Scenario | Flagyl + Augmentin | Flagyl + Ciprofloxacin | Notes |
|---|---|---|---|
| Colonic perforation | Yes | Yes | Dual coverage for anaerobes + Gram-negative aerobes |
| Abdominal abscess | Yes | Yes | Cipro added when Pseudomonas is suspected |
| Necrotizing infection | Partial | Yes | Emphasis on strong Gram-negative aerobic coverage |
| Postoperative peritonitis | Yes | Selective | Flagyl remains essential regardless of partner drug |
Augmentin is generally preferred when broad, predictable mixed-flora coverage is required.
Ciprofloxacin is useful in settings with increased risk of Pseudomonas or in patients who cannot receive β-lactams.
Modern Dosing Guidelines for Metronidazole in Abdominal Surgery (2025 Update)
Dosing strategies for Flagyl have become more standardized as stewardship principles continue to emphasize targeted therapy and avoidance of unnecessary antibiotic exposure.
Typical regimens for adults include:
- IV therapy: 500 mg every 8 hours for moderate to severe intra-abdominal infections
- Oral transition therapy: 500 mg every 8 hours once the patient is clinically improving
- Standard treatment duration: 5–7 days when adequate source control is achieved
Adjustments are necessary in specific patient groups due to differences in metabolism and drug clearance.
The following patient categories require modified dosing or closer monitoring:
- Individuals with significant hepatic impairment due to slowed metabolism
- Patients with combined hepatic and renal dysfunction receiving multiple concurrent antibiotics
- Older adults with reduced hepatic blood flow
- Patients receiving interacting medications such as warfarin or lithium
- Individuals with prior history of peripheral neuropathy undergoing prolonged therapy
While renal dysfunction alone rarely requires dosage adjustment, hepatic impairment significantly alters drug handling and must be accounted for in the perioperative plan.
Safety, Contraindications, and Drug Interactions
Although Flagyl is highly effective, surgeons must consider its key safety parameters.
The drug is contraindicated in the first trimester of pregnancy unless no safer alternative is available.
Patients with preexisting liver disease require dose reduction or extended dosing intervals due to decreased metabolic clearance.
A clinically important point is the disulfiram-like reaction associated with alcohol consumption.
Patients must be instructed to avoid alcohol during treatment and for at least 48 hours after the last dose.
Peripheral neuropathy can develop with extended courses, making symptom monitoring essential in prolonged therapy.
Drug interactions include potentiation of warfarin’s anticoagulant effect often requiring INR adjustment and elevation of lithium levels.
Coordination with pharmacy teams is often necessary to maintain safe therapeutic ranges during complex postoperative management.
Flagyl Compared With Other Anaerobic Agents (2025 Clinical Comparison)
While Flagyl remains the primary agent against obligate anaerobes in abdominal infections, surgeons must understand where alternative antibiotics may offer advantages.
Clindamycin, once considered a viable anaerobic option, has seen declining effectiveness due to rising resistance in Bacteroides fragilis.
As a result, it is no longer favored in severe abdominal infections.
Broad-spectrum β-lactam/β-lactamase inhibitor combinations, such as piperacillin/tazobactam, provide excellent mixed flora coverage and often eliminate the need for separate anaerobic agents.
However, these drugs come with higher ecological impact, broader collateral damage to microbiota, and a greater risk of resistance selection.
Carbapenems, while highly potent, are reserved for complicated or multidrug-resistant infections where narrower agents fail or resistance patterns demand escalation.
Flagyl’s enduring relevance lies in its precision.
It allows surgeons to build customized regimens that address anaerobic pathogens without unnecessarily extending Gram-negative or Gram-positive coverage.
This targeted approach aligns well with stewardship initiatives intended to reduce antibiotic pressure in surgical units.
Clinical Cases: Effective Use and Avoidable Failures
Case 1: Successful Treatment With Flagyl-Based Combination Therapy
A patient develops secondary peritonitis following sigmoid diverticular perforation.
CT imaging reveals free air and fluid accumulation, and during emergent surgery the perforated segment is resected.
Postoperatively, the antimicrobial regimen includes Flagyl paired with ciprofloxacin.
Within 48–72 hours inflammatory markers begin to decline, abdominal pain decreases, and the patient transitions to oral therapy after bowel function returns.
The rapid clinical response reflects appropriate targeting of both anaerobes and Gram-negative aerobes.
Case 2: Clinical Deterioration Following Inadequate Monotherapy
A postoperative patient with persistent fever after colorectal surgery is treated in an outpatient setting with Flagyl alone under the assumption that anaerobes are the only concern.
Within two days the patient experiences worsening abdominal pain, leukocytosis, and progressive signs of systemic inflammation.
Imaging reveals a loculated abscess containing both anaerobic organisms and Gram-negative aerobes.
Once the regimen is escalated to a full-spectrum combination, clinical improvement begins.
This scenario underscores the importance of complete microbial coverage and illustrates why modern abdominal protocols rarely rely on monotherapy.
These cases mirror observations summarized in articleHow Timely Antibiotic Therapy Reduces Amputations, where outcome improvements correlate strongly with early and appropriate antimicrobial selection, particularly in high-risk patients.
Frequently Asked Questions
Can Flagyl be used as monotherapy for abdominal infections?
No. Abdominal infections are overwhelmingly polymicrobial.
Flagyl covers anaerobes only and must be paired with an agent targeting Gram-negative aerobes.
When is Flagyl combined with Augmentin or Ciprofloxacin?
Combination therapy is recommended when perforation, abscess, or postoperative peritonitis suggests mixed aerobic–anaerobic flora.
Augmentin provides broad mixed-flora coverage; ciprofloxacin is preferred when Pseudomonas risk is high.
What is the recommended treatment duration in 2025?
Typically 5–7 days, provided that adequate source control is achieved.
Longer courses are considered only when drainage is incomplete.
Which patients require special caution when receiving Flagyl?
Patients with liver disease, those taking warfarin, individuals with prior neuropathy, and pregnant patients in the first trimester.
What is the alternative for patients who cannot tolerate metronidazole?
Alternatives include β-lactam/β-lactamase inhibitor combinations or carbapenems, depending on infection severity and microbial risk.
Sources