























The aorta is the body’s largest artery – a major highway carrying blood from the heart to every organ. When a segment of this vital vessel weakens and bulges outward like a balloon, doctors call it an abdominal aortic aneurysm, or AAA.
This condition is often called “the silent threat” because it rarely causes symptoms until it becomes life-threatening. Many people live for years with an aneurysm without realizing it, only discovering it during a routine abdominal ultrasound or CT scan performed for another reason. When the aneurysm ruptures, it can cause catastrophic internal bleeding that demands immediate surgical attention.
The goal of modern vascular medicine – and of centers like SVSA Inc. in Fishersville, VA – is to detect abdominal aortic aneurysm early, before it reaches a dangerous size. Screening, surveillance, and minimally invasive repair have transformed what was once a fatal surprise into a preventable condition.
What Is an Abdominal Aortic Aneurysm and Why Does It Develop?
An abdominal aortic aneurysm occurs when the wall of the aorta, typically below the kidneys, becomes weakened and stretches. Over time, the constant pressure of blood flow enlarges the weakened area, much like a worn spot in a garden hose.
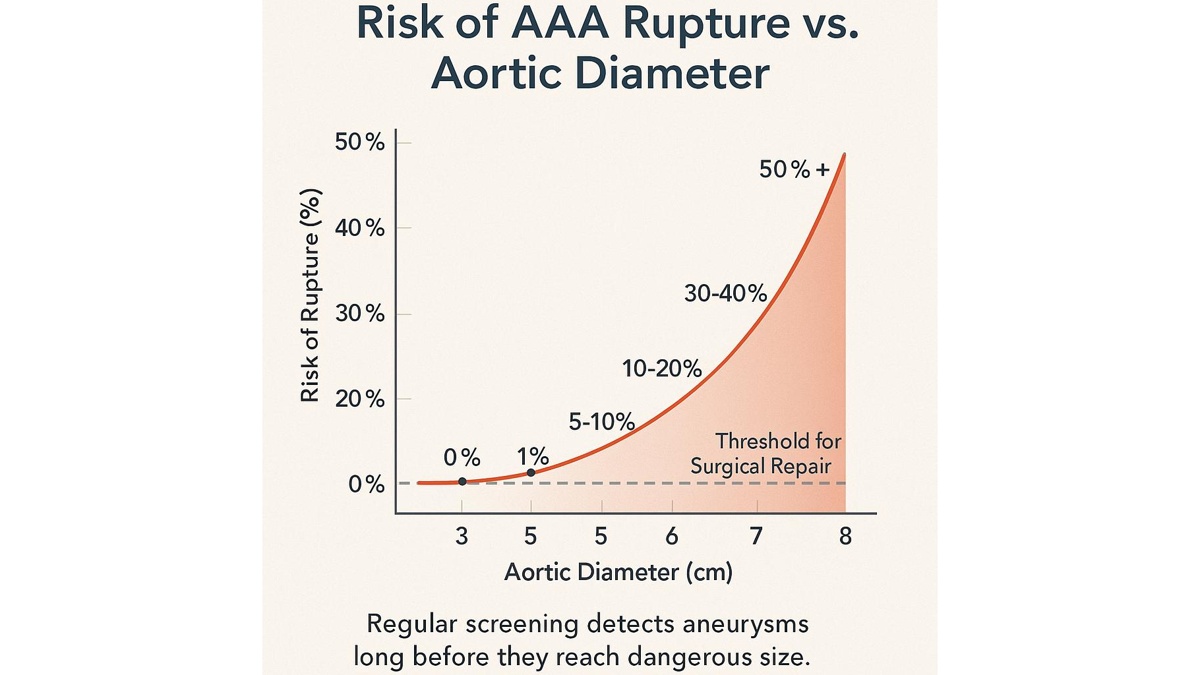
The normal diameter of the abdominal aorta in adults is about 2 cm (0.8 inches). When it expands beyond 3 cm (1.2 inches), it meets the definition of an aneurysm. The risk of rupture – and therefore of sudden death— rises sharply as the diameter increases.
How It Happens
The aortic wall is composed of three layers:
- Intima – the smooth inner lining that resists turbulence and clot formation.
- Media – the middle muscular layer that provides elasticity and strength.
- Adventitia – the outer connective layer that anchors the artery.
When the media weakens due to inflammation, genetic predisposition, or long-term exposure to toxins like cigarette smoke, it begins to lose its elastic recoil. This deterioration allows the vessel to stretch under normal blood pressure.
Microscopically, AAA is marked by the breakdown of elastin and collagen fibers – the scaffolding that keeps the artery stable. Chronic inflammation further erodes these fibers, leading to progressive dilation.
Silent Progression
Most AAAs grow slowly and silently. Patients rarely feel pain or notice any change. In some cases, a pulsating mass may be felt in the abdomen, but this is uncommon. The danger lies in the unpredictability of rupture: when the wall can no longer withstand the pressure, it tears suddenly, leading to rapid internal bleeding. Without emergency surgery, survival rates drop below 20%.
Why It’s Often Missed
Because abdominal aortic aneurysm usually causes no symptoms, it’s often discovered by accident — during imaging for kidney stones, back pain, or routine wellness scans. For this reason, vascular specialists strongly recommend screening ultrasound for individuals at risk, especially older men and long-term smokers.
Early detection through abdominal aortic aneurysm screening can reduce mortality by more than 40%, according to multiple U.S. and international studies. The ultrasound test is quick, painless, and widely available — a few minutes that can literally save a life.
The Anatomy of Risk
The location of the aneurysm also matters.
- Infrarenal AAA (below the kidneys) is the most common type, accounting for about 80% of cases.
- Juxtarenal or suprarenal AAA (involving the kidney arteries) is more complex and may require advanced endovascular techniques.
No matter the site, the principle is the same: once the aortic wall begins to dilate, ongoing monitoring or treatment is essential to prevent rupture.
Key Risk Factors: Smoking, Age, and Family History
Although anyone can develop an abdominal aortic aneurysm, certain factors dramatically raise the risk. Understanding these is crucial for prevention and early diagnosis.
Smoking
Smoking is by far the leading cause of AAA formation and rupture. The toxins in tobacco accelerate the breakdown of elastin and collagen in the aortic wall, weakening it over time. Smokers are up to five times more likely to develop an aneurysm than non-smokers. Even after quitting, the damage may persist – another reason early screening is essential for anyone with a smoking history.
Age and Gender
Age is the second strongest predictor. Most AAAs occur in people over 65 years old, and the risk increases steadily with each decade of life. Men are affected far more often than women, although women with aneurysms tend to face higher rupture risk once the condition develops.
Because of this, U.S. guidelines – including those followed at SVSA Inc. in Fishersville, VA — recommend a one-time abdominal ultrasound for:
- Men aged 65–75 who have ever smoked
- Men or women over 65 with a family history of AAA
Family History and Genetics
If a parent, brother, or sister has had an aortic aneurysm, your risk roughly doubles. In such cases, screening may start earlier around age 55. Certain inherited connective-tissue disorders (like Marfan or Ehlers-Danlos syndromes) also predispose patients to aneurysmal disease.
High Blood Pressure and Atherosclerosis
Chronic hypertension and plaque buildup strain the arterial wall, promoting aneurysm growth. Managing blood pressure and cholesterol is therefore one of the most effective ways to prevent expansion after diagnosis.
Other Contributing Conditions
- Chronic lung disease — reduces oxygen delivery to tissues, impeding vascular repair
- Inflammatory aortitis — causes localized vessel wall injury
- Male sex hormones (testosterone) — may influence collagen metabolism and vessel elasticity
Early imaging is justified even in the absence of symptoms, especially when multiple risk factors overlap.
How AAA Screening Works at SVSA (Fishersville, VA)
At SVSA Inc., screening for abdominal aortic aneurysm is a simple, non-invasive procedure that can be completed in about 15 minutes. It’s painless, safe, and highly accurate.
The Process
- Preparation — Patients are asked to fast for 4–6 hours to reduce intestinal gas that might obscure the image.
- Ultrasound Examination — A technician applies gel to the abdomen and uses a transducer to capture real-time images of the aorta.
- Measurement — The diameter of the abdominal aorta is measured in several locations.
- Results — The vascular surgeon reviews the images, determines if an aneurysm is present, and provides follow-up recommendations on the spot.
Advantages of Ultrasound Screening
- Completely radiation-free
- Highly sensitive — detects nearly all aneurysms ≥ 3 cm
- Quick — results available immediately
- Affordable and accessible — especially important in community-based vascular care centers like SVSA
For many patients, this is their first step toward proactive vascular management. When caught early, small aneurysms can be safely monitored for years before intervention becomes necessary.
Aortic Diameter, Condition, and Recommended Follow-Up
| Aortic Diameter | Condition | Recommended Action |
|---|---|---|
| < 3 cm | Normal | Repeat ultrasound in 5 years |
| 3 – 4.4 cm | Small aneurysm | Ultrasound every 12 months |
| 4.5 – 5.4 cm | Medium aneurysm | Ultrasound every 6 months |
| ≥ 5.5 cm | High-risk aneurysm | Surgical repair recommended |
This table reflects current Society for Vascular Surgery (SVS) guidelines and helps standardize care. The goal is clear: detect aneurysms before they rupture and intervene only when the benefits outweigh surgical risks.
Treatment Options: Endovascular and Open Surgery
Once an abdominal aortic aneurysm reaches a critical size or begins to grow rapidly, surgical repair becomes necessary to prevent rupture. The choice between endovascular and open repair depends on the aneurysm’s size, shape, and the patient’s overall health.
Endovascular Aneurysm Repair (EVAR)
EVAR is a minimally invasive technique and is now the preferred approach for most patients. Through small incisions in the groin, the vascular surgeon inserts a catheter into the femoral artery and guides it to the aneurysm. A stent graft — a fabric-covered metal tube — is then positioned inside the weakened aorta.
Once in place, the graft seals off the aneurysm from blood flow, reducing pressure on the vessel wall and preventing rupture.
Advantages of EVAR
- Small incisions and faster recovery (usually 1–2 days in hospital)
- Lower immediate risk of complications compared to open surgery
- Suitable for older patients or those with multiple medical conditions
Limitations
- Requires regular imaging follow-up to check graft position
- Not ideal for all anatomical shapes of aneurysms
- Possible need for secondary procedures if small leaks (“endoleaks”) occur
Open Surgical Repair
Open repair remains the gold standard for patients who cannot undergo EVAR or for aneurysms that are anatomically complex. During open surgery, the surgeon makes an incision in the abdomen, clamps the aorta above and below the aneurysm, removes the diseased segment, and replaces it with a durable synthetic graft.
While recovery takes longer (about 1–2 weeks in hospital), open repair provides a permanent solution in most cases. The graft does not require the same level of long-term imaging surveillance as EVAR.
Open repair may be preferred when:
- The aneurysm extends near or above the kidneys
- The aorta is too tortuous for a stent graft
- The patient is relatively young and fit
At SVSA Inc., vascular surgeons are trained in both techniques, ensuring each patient receives the safest and most effective treatment for their specific anatomy and health profile.
Prevention and Monitoring After Diagnosis
Even after diagnosis or treatment, vascular care remains a lifelong commitment. Prevention focuses on slowing aneurysm growth and reducing rupture risk.
Regular Imaging
After diagnosis of a small aneurysm, routine ultrasound or CT scans track growth:
- Every 12 months for aneurysms 3–4.4 cm
- Every 6 months for aneurysms 4.5–5.4 cm
- More frequent scans if rapid expansion (>0.5 cm/year) occurs
These intervals are based on Society for Vascular Surgery (SVS) recommendations and ensure timely surgical planning if necessary.
Blood Pressure Control
Hypertension accelerates aneurysm expansion. Keeping blood pressure below 130/80 mmHg with medication, diet, and exercise significantly lowers stress on the aortic wall.
Smoking Cessation
No single lifestyle change is more important. Quitting smoking not only slows aneurysm growth but also improves surgical outcomes and graft longevity.
Cholesterol and Weight Management
A diet low in saturated fats and rich in fruits, vegetables, and whole grains supports vascular integrity. Weight loss reduces overall arterial strain and inflammation.
Regular Follow-Up with a Vascular Surgeon
After surgery — whether EVAR or open — annual or semiannual imaging ensures the repair remains stable. Many patients live decades after successful repair when follow-up is maintained.
Call to Action: Schedule an Aortic Ultrasound at SVSA
Abdominal aortic aneurysm is a silent but preventable condition. A quick, painless ultrasound can identify early-stage aneurysms long before symptoms appear.
If you are over 65, have ever smoked, or have a family history of aneurysms, don’t wait. Screening at SVSA in Fishersville, VA provides peace of mind and a clear plan for your vascular health.
F.A.Q
What is an aortic aneurysm?
An aortic aneurysm is a bulging or enlargement of the body’s main artery, the aorta. When it occurs in the abdomen, it’s called an abdominal aortic aneurysm (AAA). If it ruptures, it causes life-threatening internal bleeding.
How can I know if I have it if there are no symptoms?
Most people with aortic aneurysm have no symptoms. The only way to detect it early is through an ultrasound screening. The test is quick, safe, and can detect aneurysms as small as 3 cm.
How dangerous is an aortic aneurysm rupture?
Extremely dangerous. Once the aneurysm ruptures, the survival rate drops below 20%. That’s why early detection and preventive surgery are crucial.
How should I prepare for an abdominal ultrasound?
Avoid eating or drinking for 4–6 hours before the test. This reduces intestinal gas and allows a clearer image of your aorta. You can take regular medications with a sip of water unless your doctor advises otherwise.
Can I live with an aneurysm without surgery?
Yes, if the aneurysm is small and stable. Many patients live safely for years with careful monitoring, blood pressure control, and regular imaging. Surgery is only needed if the aneurysm grows or exceeds 5.5 cm in diameter.
Author:
Dr. Charles D. Goff, MD, FACS

Sources
- Society for Vascular Surgery (SVS) – Abdominal Aortic Aneurysm
- Centers for Disease Control and Prevention (CDC) – Aortic Aneurysm Facts
- National Heart, Lung, and Blood Institute (NHLBI) – Aortic Aneurysm Treatment
- U.S. Preventive Services Task Force (USPSTF) – Abdominal Aortic Aneurysm Screening
- Mayo Clinic – Abdominal Aortic Aneurysm: Diagnosis and Treatment (2024 Update)