























Doxycycline’s Role in Surgical Antibiotic Therapy
Disclaimer
This article is intended for informational purposes and does not constitute medical advice. Antibiotic therapy must be prescribed only after direct evaluation by a qualified healthcare professional. Inaccurate or self-directed antibiotic use may lead to complications or treatment failure.
Author: Donald C. Carmichael, MD
Why Doxycycline Became a Key β-Lactam Alternative in 2025
In 2025, doxycycline occupies a central place among alternative antibiotics for patients with β-lactam allergy. Surgeons increasingly encounter individuals with confirmed hypersensitivity to penicillins and cephalosporins, which limits the use of standard postoperative regimens. Doxycycline fills this gap because it provides clinically meaningful activity against pathogens frequently responsible for postoperative soft-tissue infections, including community-acquired MRSA.
Unlike many substitutes, doxycycline combines broad antimicrobial utility with excellent oral bioavailability, allowing it to function effectively as a postoperative antibiotic for ambulatory surgical patients. Its favorable safety profile and predictable tissue penetration make it one of the most practical options when a β-lactam cannot be used. For this reason, doxycycline has become a routine component of surgical prescribing algorithms, particularly in outpatient wound management and minor postoperative complications.
Spectrum of Activity and Relevance in Surgical Practice
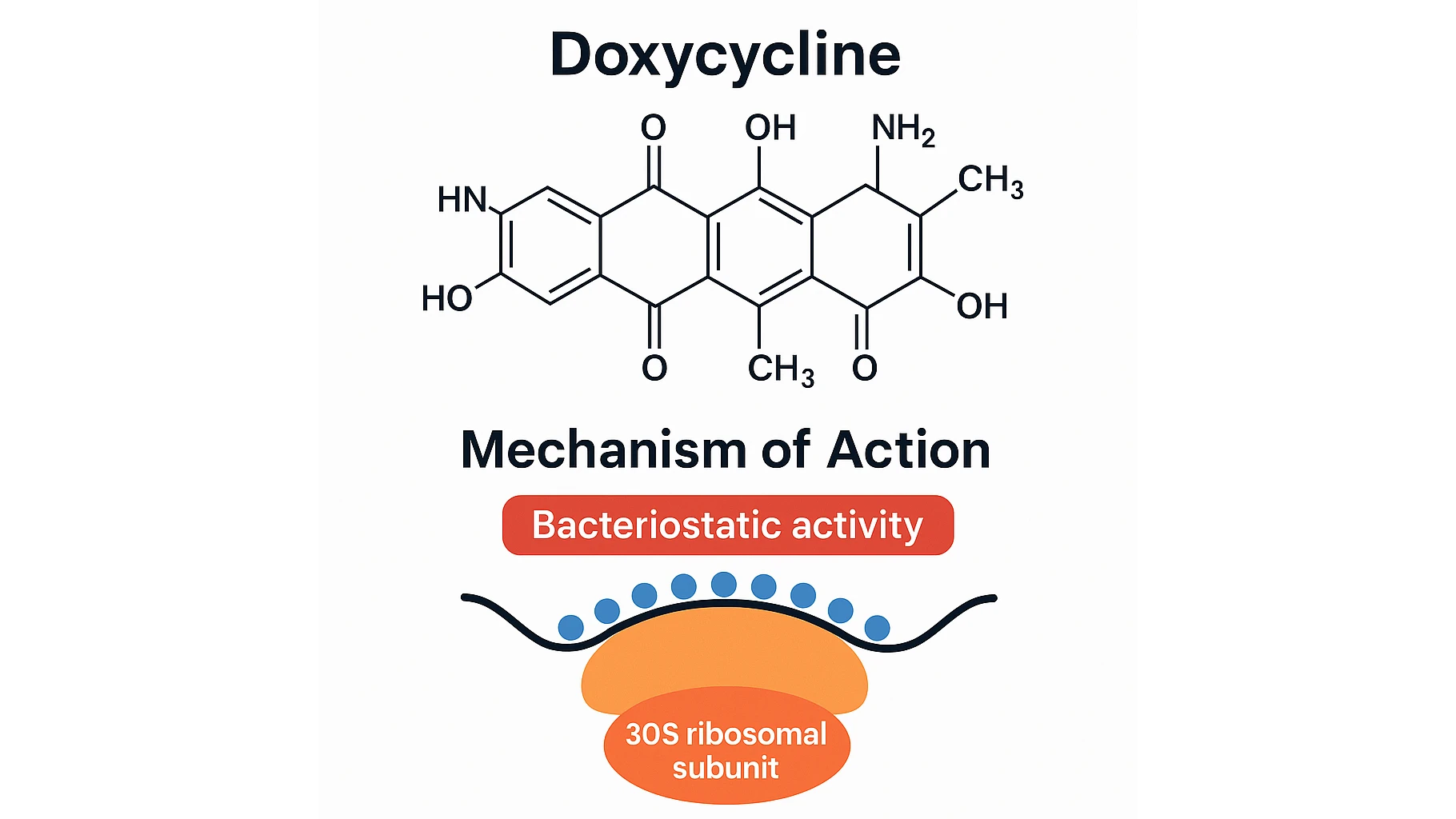
Doxycycline inhibits bacterial protein synthesis by binding to the 30S ribosomal subunit, giving it reliable action against MSSA, MRSA, atypical organisms, and several Gram-negative pathogens. These features explain why clinicians select doxycycline for surgical infections that involve staphylococcal species or in cases where the patient requires an effective non–β-lactam alternative.
Its limitations are equally important. Doxycycline has reduced activity against Streptococcus pyogenes and does not cover anaerobic bacteria, which restricts its use in abdominal infections and deep contaminated wounds. Nevertheless, for many superficial or moderate postoperative infections such as cellulitis, suture irritation, and minor surgical-site inflammation doxycycline remains a strong evidence-based choice. Compared with macrolides discussed in article Azithromycin in Surgery, doxycycline offers more reliable staphylococcal coverage, which is essential in postoperative soft-tissue care.
When Doxycycline Is the Correct Substitute for β-Lactams
Doxycycline is appropriate when a patient presents with a documented IgE-mediated β-lactam reaction, including anaphylaxis, urticaria, or severe delayed hypersensitivity. In these cases, avoiding β-lactams is a safety priority, and doxycycline becomes a primary alternative.
Doxycycline is particularly suitable when:
- the likely pathogen includes MRSA or MSSA;
- postoperative inflammation is limited to soft tissue without anaerobic involvement;
- the patient requires a well-tolerated oral antibiotic for outpatient recovery;
- culture results support susceptibility;
- β-lactam options are contraindicated due to prior reactions.
This aligns with postoperative treatment strategies described in article Postoperative Antibiotic Therapy, where short targeted courses are preferred over broad-spectrum regimens whenever possible.
When Doxycycline Should NOT Be Used
Although doxycycline has earned a strong position as a β-lactam alternative, its limitations remain critical in surgical practice. The drug provides unreliable coverage against Group A Streptococcus, making it a poor choice for infections where streptococcal dominance is suspected. It also lacks activity against anaerobes, which excludes its use in abdominal infections, perineal wounds, or any scenario involving bowel contamination.
Doxycycline is similarly inappropriate for severe or rapidly progressing postoperative infections, especially in immunocompromised patients or those at risk for bacteremia. In these cases, broader-spectrum agents or intravenous therapy may be required. Pediatric patients under eight years of age and pregnant patients should not receive doxycycline due to risks of tooth discoloration and potential effects on bone development.
Because these contraindications directly affect postoperative decision-making, surgeons often return to structured antibiotic-selection frameworks such as those described in article How a Surgeon Actually Chooses the Right Antibiotic in 2025, which outlines clinical algorithms for selecting agents based on risk factors, comorbidities, and infection patterns.
Doxycycline Compared With Keflex, Azithromycin, and Bactrim
In surgical infections, doxycycline is rarely evaluated in isolation. Surgeons routinely compare it with other non–β-lactam options to ensure that the antibiotic chosen aligns with microbial risk and anatomical context.
Compared with Keflex (cephalexin)
Doxycycline provides superior coverage of MRSA, which makes it a better choice for postoperative wound infections in patients with known staphylococcal colonization or previous MRSA history. Keflex remains preferred for streptococcal infections, but cannot serve as an alternative when β-lactam allergy is present.
Compared with azithromycin
As noted in v Azithromycin in Surgery, azithromycin lacks reliable action against MSSA and MRSA, limiting its usefulness in surgical-site infections. Doxycycline provides far more dependable staphylococcal coverage, which is why it is chosen more frequently in postoperative soft-tissue care.
Compared with Bactrim (TMP-SMX)
Both doxycycline and Bactrim have activity against MRSA. Doxycycline is often chosen when gastrointestinal tolerability is a priority, or when a simpler dosing schedule is needed. Bactrim may be preferred when Gram-negative coverage is desirable, but its interaction profile and risk of hypersensitivity are more restrictive.
These differences explain why doxycycline is consistently included in postoperative antibiotic alternatives when β-lactams are contraindicated, particularly for mild to moderate surgical infections of the skin and soft tissues.
Drug Interaction Table (2025 Update)
Doxycycline remains widely used because of its simplicity, but several clinically significant drug interactions must be considered during surgical treatment. The table below summarizes the most relevant interactions for perioperative care.
| Drug Class | Interaction Mechanism | Clinical Effect | Recommendation |
|---|---|---|---|
| Antacids, calcium, magnesium | Chelation reduces absorption | Subtherapeutic antibiotic levels | Separate doses by 2–3 hours |
| Warfarin | Potentiation of anticoagulant effect | Elevated INR, bleeding risk | Monitor INR closely |
| Retinoids (e.g., isotretinoin) | Increased intracranial pressure | Headache, visual changes | Avoid combination |
| Barbiturates, carbamazepine | Enzyme induction | Lower doxycycline concentration | Adjust dose if needed |
| Oral contraceptives | Reduced contraceptive reliability | Unintended pregnancy risk | Recommend backup contraception |
These interactions highlight the importance of reviewing medications during postoperative follow-up, especially in patients already taking anticoagulants or antacids.
Dosing Recommendations and Duration in 2025
Modern guidelines emphasize structured dosing to achieve reliable therapeutic concentrations while minimizing toxicity. Standard dosing for adults is doxycycline 100 mg once or twice daily, with the twice-daily regimen preferred for active postoperative infections. A loading dose may be used in situations requiring rapid therapeutic onset, such as early postoperative cellulitis or MRSA-associated wound inflammation.
Duration depends on severity, surgical site, and presence of comorbidities:
- Uncomplicated soft-tissue infections: 5–7 days
- Confirmed MRSA involvement: 7–10 days
- Postoperative inflammatory flare without purulence: typically 3–5 days
- Deeper infections requiring prolonged suppression: individualized based on response
Doxycycline dosing strategies often mirror the treatment durations discussed in article Postoperative Antibiotic Therapy, where optimized postoperative antibiotic duration plays a critical role in reducing complications and preventing overtreatment.
Safety Profile and Contraindications
Doxycycline is generally well tolerated, which contributes to its widespread adoption as a non–β-lactam postoperative antibiotic. Nevertheless, several safety considerations remain important in surgical care.
The most common adverse effects involve gastrointestinal discomfort and photosensitivity. The latter is particularly relevant for patients undergoing outpatient dermatologic and plastic procedures, as postoperative sun exposure can worsen inflammatory reactions. Surgeons must advise patients to avoid direct sunlight and use sunscreen while receiving doxycycline.
A less frequent but clinically significant risk is esophagitis. Because the drug can cause mucosal irritation, patients should be instructed to take doxycycline with a full glass of water and remain upright for at least 30 minutes after ingestion.
Rare toxicities—such as increased intracranial pressure or hepatotoxicity—typically appear in patients receiving prolonged courses or using interacting medications. For this reason, long-term therapy should be reserved for select cases and always monitored carefully.
Clinical Scenarios: Appropriate and Inappropriate Use
Case 1: Appropriate Use in β-Lactam Allergy With MRSA Risk
A patient with a documented β-lactam allergy undergoes outpatient excision of a lipoma. On postoperative day three, mild erythema and tenderness develop around the incision. Because the patient has a history of MRSA colonization, doxycycline is selected as a targeted oral agent. Within 48 hours inflammation begins to resolve, and the patient completes a seven-day course without complications. This scenario reflects the exact setting where doxycycline provides an optimal balance of safety and efficacy.
Case 2: Incorrect Use in a Mixed Anaerobic Infection
A middle-aged patient develops postoperative abdominal discomfort after colon surgery. Purulent drainage suggests a deeper infection involving anaerobic organisms. Despite this, doxycycline is started empirically due to β-lactam allergy. Over the next 24 hours symptoms worsen because the drug provides no anaerobic coverage. Once therapy is switched to an appropriate combination that includes anti-anaerobic activity, clinical improvement follows. This case demonstrates why doxycycline should not be used for abdominal infections or any situation involving suspected anaerobes.
Case 3: Combined Therapy in a Complex Soft-Tissue Infection
A patient presents with a postoperative soft-tissue infection complicated by mild immunosuppression. Cultures show MRSA and a susceptible Gram-negative organism. Doxycycline is included in a combination regimen to improve staphylococcal coverage while maintaining oral treatment feasibility. The infection resolves with close follow-up and proper adherence.
These examples mirror broader surgical trends described in article №15, where timely and appropriate antibiotic selection significantly reduces postoperative complications and improves limb-salvage and recovery outcomes.
Frequently Asked Questions
Can doxycycline be used after surgery?
Yes, doxycycline is a suitable postoperative antibiotic for selected soft-tissue infections, particularly when β-lactams are contraindicated.
Is doxycycline effective against MRSA in 2025?
Yes. It remains a reliable oral option for community-acquired MRSA in mild to moderate surgical infections.
What if the patient takes antacids or supplements?
These agents reduce doxycycline absorption. Doses must be separated by several hours to maintain therapeutic levels.
Can doxycycline replace Augmentin?
Only in situations where anaerobes are not suspected. Doxycycline cannot substitute for Augmentin in abdominal or polymicrobial infections.
How long should postoperative doxycycline therapy continue?
Most superficial infections respond within 5–7 days. MRSA-related infections may require 7–10 days, depending on the clinical picture.