























Keflex in Modern Surgery
Medical Disclaimer
This article is intended for educational and clinical review purposes only. It should not replace direct surgeon-to-patient evaluation, microbiology consultation, or hospital-specific antimicrobial protocols.
Author: Charles D. Goff, MD, FACS
Why Keflex Still Matters in Surgical Practice (2025 Update)
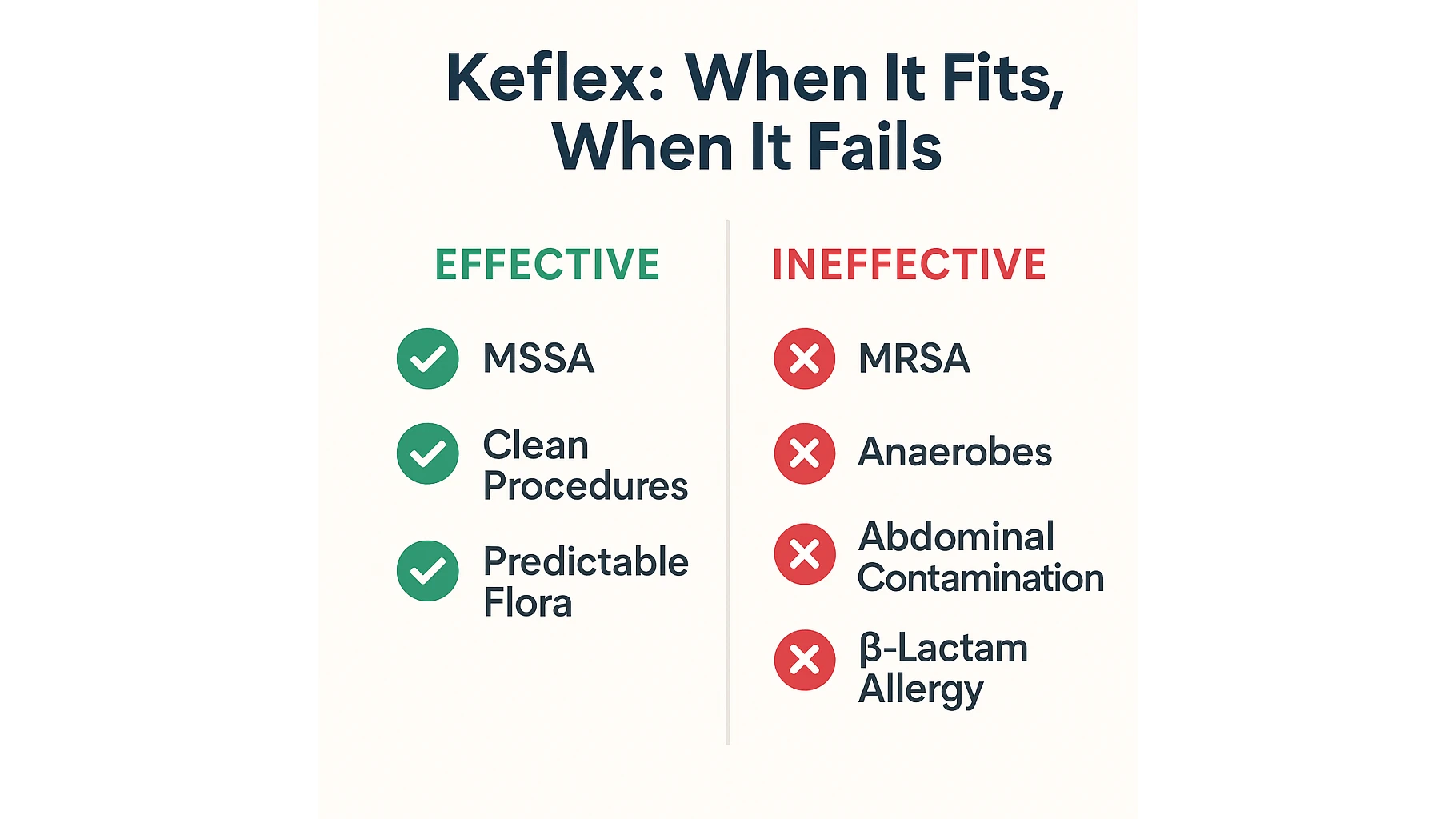
Keflex (cephalexin) continues to hold an important place in surgical care in 2025, even as antibiotic stewardship has become significantly more stringent. Its relevance stems from the fact that the majority of surgical site infections (SSI) following clean procedures are still caused by predictable Gram-positive organisms primarily methicillin-sensitive Staphylococcus aureus (MSSA) and various Streptococcus species.
Because cephalexin targets these organisms reliably, it remains a preferred agent when broad-spectrum coverage is unnecessary or potentially harmful.
A growing number of 2024–2025 guideline updates emphasize that prophylaxis should match the microbial environment rather than default to expansive regimens. Keflex’s narrow spectrum works to the surgeon’s advantage in these scenarios: it reduces collateral damage to the patient’s microbiome, minimizes the risk of Clostridioides difficile infection, and decreases selective pressure that drives resistance in hospital settings.
These principles align with modern stewardship goals, which push clinicians to avoid broad-spectrum antibiotics unless the clinical situation clearly demands them.
Cephalexin’s ease of use also supports its continued popularity. It is well tolerated, cost-effective, and available in oral formulations that allow a smooth perioperative transition.
Patients undergoing minor and moderate procedures can continue the same antibiotic after discharge without the complexity of switching to different oral alternatives. This contributes to better adherence an often underestimated factor in SSI prevention.
In 2025, surgeons are not looking for “a strong antibiotic” they are looking for the right antibiotic. And for clean, low-risk operations, Keflex still fits that definition.
When Keflex Is the Optimal Choice for Surgeons (Evidence-Based Indications)
Although clinical practice is shifting toward more personalized antibiotic strategies, Keflex remains a first-line option whenever the expected pathogens match its activity spectrum.
Clean soft-tissue operations are the clearest example. Procedures such as excision of benign lesions, removal of small subcutaneous masses, revision of minor scars, or closure of uncomplicated lacerations typically expose the surgical field only to the patient’s skin flora.
In these settings, MSSA and streptococci dominate, and cephalexin’s targeted action is not only sufficient but optimal.
Modern SSI studies consistently show no benefit in using broader antibiotics for these procedures. In fact, switching to broad-spectrum agents tends to increase the rate of gastrointestinal side effects without improving infection outcomes.
By contrast, Keflex provides a balance of safety, narrow spectrum, and proven efficacy in low-contamination surgical fields.
The drug also performs well in minor traumatic injuries that require operative repair but do not involve contaminated environments such as soil, feces, bite wounds, or chronic ulcers.
When surgeons can confidently predict that Gram-positive organisms represent the main microbial threat, cephalexin is appropriate and avoids overtreatment.
Another advantage is its integration into perioperative workflows. Because it is commonly used for both prophylaxis and short postoperative courses, it reduces the number of medications patients must learn and follow an especially useful feature in ambulatory surgery centers and outpatient wound care.
When Keflex Is Weak, Unsafe, or Clinically Inappropriate
Despite its strengths, Keflex has several important limitations that surgeons must recognize to avoid postoperative complications.
The most significant is its complete lack of activity against MRSA. Although MRSA prevalence varies among regions and patient populations, colonization remains common enough that surgeons must assess MRSA risk before relying on cephalexin.
Using Keflex in a patient with known or suspected MRSA colonization significantly increases the likelihood of treatment failure.
Another major limitation is its inability to treat anaerobic organisms. This issue becomes critical in gastrointestinal surgery, trauma involving the abdomen or pelvis, and any procedure where bowel contamination is possible.
Anaerobes play a central role in these infections, and cephalexin cannot address them.
This is precisely why surgeons frequently rely on agents like Flagyl when managing abdominal or pelvic infections an approach discussed in more depth in Article Flagyl (Metronidazole) for Anaerobic Abdominal Infections
The transition feels natural in modern guidelines: cephalexin for clean cases, but a dedicated anaerobic agent whenever the surgical field involves the gastrointestinal tract.
Keflex is also not appropriate for infections requiring broad Gram-negative coverage, such as vascular graft infections, diabetic foot infections, or deep limb-threatening soft-tissue infections.
These conditions are often polymicrobial, and cephalexin’s narrow spectrum leaves major gaps that can worsen patient outcomes.
Finally, while true cephalosporin allergies are uncommon, clinicians must still exercise caution in patients with a documented severe reaction to β-lactams. Even though cross-reactivity is lower than once believed, the risk is not zero, and alternative agents are often safer.
Modern Keflex Dosing Standards in Surgical Care
Keflex dosing in 2025 follows a disciplined, evidence-based approach that prioritizes targeted exposure over prolonged or broad-spectrum coverage.
A single 2-gram oral dose administered 60 minutes before incision remains the standard for preoperative prophylaxis, supported by recent multicenter studies demonstrating that timing is the principal determinant of prophylactic effectiveness.
Postoperative use has been shortened significantly over the last decade.
For clean and moderately contaminated procedures, cephalexin is rarely continued beyond 24–48 hours, as extending therapy has not shown additional benefit in reducing SSI rates.
When treating confirmed MSSA soft-tissue infections, therapeutic dosing typically ranges from 500 to 1,000 mg every six hours, with routine adjustment in patients with impaired renal function.
Keflex Dosing Summary (2025)
| Clinical Use Case | Dose | Frequency | Typical Duration | Notes |
|---|---|---|---|---|
| Preoperative prophylaxis | 2 g | once | — | Administer 60 minutes before incision |
| Postoperative prophylaxis | 500 mg | q6–8h | 24–48 h | Longer courses discouraged |
| MSSA soft-tissue infection | 500–1000 mg | q6h | 5–7 days | Only with low MRSA risk |
| Renal impairment | adjusted | — | — | Reduce dose per eGFR |
Contraindications, Safety Considerations, and Adverse Effects
Although Keflex is generally safe, appropriate patient selection remains essential in surgical practice.
Severe β-lactam hypersensitivity continues to be the primary contraindication, particularly in patients with a history of anaphylaxis.
Cephalexin requires cautious dosing in individuals with reduced renal function, as accumulation can occur when clearance is diminished.
Common adverse effects:
- mild gastrointestinal discomfort
- transient diarrhea
- uncomplicated skin eruptions
Rare but clinically important reactions:
- serum sickness–like responses
- severe cutaneous hypersensitivity
- systemic allergic reactions requiring discontinuation
Postoperative complaints must be evaluated carefully, as distinguishing expected medication-related symptoms from early infection remains crucial for correct management.
The 2025 Surgical Decision Framework: When Keflex Is the Right Choice
Antibiotic selection now follows a structured decision model grounded in microbial risk assessment.
Before prescribing cephalexin, surgeons typically evaluate the likelihood of MRSA involvement, the contamination level of the surgical field, the probability of anaerobic participation, the patient’s β-lactam tolerance, and whether renal function allows for standard dosing.
When these variables support its use, Keflex remains an appropriate and effective choice for many clean and low-risk procedures.
Over the past decade, numerous postoperative complications have been traced not to emerging resistance but to errors in initial antibiotic selection.
These missteps are highlighted in several surgical case analyses, including the clinical error patterns described in article №6, where inappropriate reliance on cephalexin was shown to contribute directly to avoidable infections.
Comparative Analysis: Keflex vs Augmentin, Bactrim, and Doxycycline
As surgical antibiotic strategies become more individualized, surgeons frequently compare Keflex with other commonly used agents.
Each alternative covers different gaps in cephalexin’s spectrum, and understanding these distinctions is essential when tailoring prophylaxis or treatment.
Augmentin offers broader coverage, particularly for mixed aerobic–anaerobic infections, making it suitable for operations involving the oropharynx, perineum, or contaminated soft tissues.
Bactrim delivers reliable MRSA coverage but is less effective against streptococcal species, which limits its role in routine surgical prophylaxis.
Doxycycline carries activity against community-acquired MRSA and has favorable oral bioavailability, but its limited streptococcal coverage and gastrointestinal tolerability issues narrow its application.
Spectrum and Clinical Role Comparison (2025)
| Antibiotic | MSSA | MRSA | Anaerobes | Gram-Negatives | Typical Surgical Use |
|---|---|---|---|---|---|
| Keflex | Excellent | None | None | Limited | Clean soft-tissue procedures |
| Augmentin | Excellent | Partial | Good | Moderate | Contaminated or mixed infections |
| Bactrim | Moderate | Excellent | None | Good | MRSA-risk patients |
| Doxycycline | Moderate | Excellent | None | Limited | MRSA soft-tissue infections |
This comparison highlights why Keflex remains trustworthy in predictable Gram-positive environments but requires substitution when anaerobes, Gram-negative rods, or MRSA are involved.
Clinical Case Examples: Successes and Pitfalls in Keflex Use
Case-based evidence remains one of the most instructive ways to understand the antibiotic’s strengths and weaknesses in real surgical practice.
Successful Application
A typical scenario involves a patient undergoing excision of a benign skin lesion in a clean operative field.
Preoperative cephalexin, timed appropriately, provides sufficient prophylaxis against MSSA and streptococcal organisms.
In follow-up, the incision heals without erythema, drainage, or signs of infection.
This reflects the clinical environments where Keflex truly excels low contamination, predictable flora, and absence of MRSA risk.
Misapplication and Complications
Contrast this with a patient presenting after a traumatic laceration contaminated with soil and debris.
Despite the presence of anaerobic risk factors, the initial provider prescribes cephalexin.
Within 48 hours, the wound shows spreading cellulitis and foul-smelling drainage, prompting reassessment and initiation of broader-spectrum therapy.
This case mirrors patterns frequently observed in surgical adverse-event analyses: misjudgment of contamination level or bacterial composition leads to inappropriate reliance on a narrow-spectrum agent.
These examples reinforce a central principle of 2025 surgical stewardship: Keflex works exceptionally well when the microbiology is predictable and fails quickly when it is not.
Frequently Asked Questions
Does Keflex treat MRSA?
No. Cephalexin does not cover MRSA, and it should not be used when MRSA colonization or infection is suspected.
Can patients with penicillin allergies safely take Keflex?
It depends on the type of allergy. Non–IgE-mediated reactions often allow cephalexin use, while any history of anaphylaxis warrants caution and usually exclusion.
How long should Keflex be taken after surgery in 2025?
For most clean or moderately contaminated procedures, 24–48 hours is sufficient. Longer courses have not shown improved outcomes.
Is Keflex appropriate for abdominal or anaerobic infections?
No. It has no anaerobic activity and should be replaced with an agent suited to intra-abdominal environments.
When should a surgeon choose Augmentin or Bactrim instead of Keflex?
Augmentin is preferred when anaerobes or mixed flora are expected. Bactrim is used when MRSA is a concern.